Audio clip: Adobe Flash Player (version 9 or above) is required to play this audio clip. Download the latest version here. You also need to have JavaScript enabled in your browser.
[Direct Download Podcast MP3]
- Simon Laing
- Andy Neill
- Nikki Abela
- Craig Davidson
Welcome back to our 2nd monthly literature review podcast. We’ve had positive feedback on the first one but we’re always keen to get better so be sure to let us know what you think through or the comments or even .
Paper Number 1
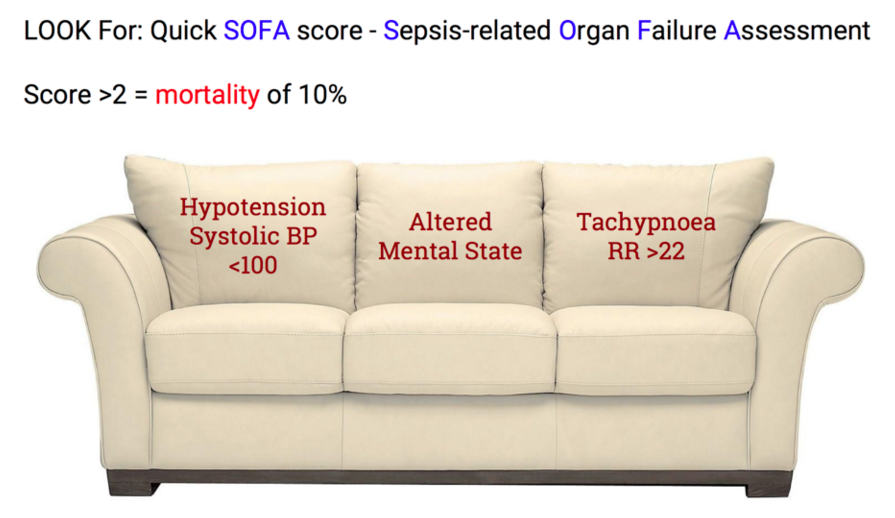
Just when you thought you had sepsis all sorted they go and change the definitions on you.

Click to go to PubMed
This is a huge topic and really complicated. Even the definitions come in a trio of 3 papers, with the first being the one covered here and two others one looking at how they defined the definitions, the clinical criteria and how they retrospectively tested it.
The bottom line(s)
- Sepsis: life-threatening organ dysfunction due to a dysregulated host response to infection
-
Septic Shock: is a subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality.
- Septic shock clinical criteria:
- Sepsis and (despite adequate volume resuscitation) both of:
- Persistent hypotension requiring vasopressors to maintain MAP greater than or equal to 65 mm Hg, and
- Lactate greater than or equal to 2 mmol/L
- With these criteria, hospital mortality is in excess of 40% (via LITFL)
- Septic shock clinical criteria:
- SIRS is out and qSOFA and SOFA are in as being more appropriate tools for identifying/screening for sepsis
via EM3 (click for source)
Is this going to change what you do? Let us know
Further Reading:
- FOAMCast
- St Emlyns
- First 10EM
- PulmCrit
- LITFL
- REBEL EM
- EM3
- Kaukonen et al 2015: SIRS misses 1 in 8 with sepsis
- Shankar-Hari et al 2016: The methods behind the sepsis definitions
- JAMA Podcast on sepsis definitions
- JAMASepsis.com JAMA made a whole website to help explain things.
Paper Number 2

Click to go to PubMed
1973 patients of an eligible 4187 being admitted to 16 hospitals in Norway with ACS or unstable angina. The invasive arm received angiogram +/- PCI/CABG while the control received optimal medical therapy. The outcome assessed was a composite Composite of MI, need for revascularisation (increasing angina despite optimum medical treatment as judged by the clinician), stroke & death.
There was a 20% absolute risk reduction of the composite outcome favouring the invasive strategy. This benefit was largely made up of reduced recurrent MI and there was no benefit in terms of mortality.
Paper Number 3

Click to go to PubMed
This paper looked at 70 patients with probably migraine in turkey. Randomised to either dexamethasone/metoclopramide versus 1g Magnesium IV. Primary outcome was a pain scale at 2 hrs. Small numbers, no clear allocation concealment and unclear how people were selected. Another option for migraine management though 2 prior trials were so so when studied
Further Reading:
Paper Number 4

Click to go to PubMed
This diagnostic paper enrolled Italian ED patients with SOB to see if Lung US was better than clinical work up alone for the diagnosis of heart failure.
Results
- 1000 pts
- 50% had heart failure overall
- ultrasound assisted diagnostic approach: sensitivity 97%, specificity 97%
- usual clinical work up: sensitivity 85%, specificity 90%
- also found great agreement on the presence of B lines between novice and expert operators
Further Reading:
- 5 Minute Sono
- Ultrasound podcast
- LITFL Review (original source)
Paper Number 5

Click to go to PubMed
This study looked at the use of the Low Risk Ankle rule which basically says in children (ages 3-16) with an acute ankle injury (<72 hours) if the tenderness and swelling is limited to distal fibular and/or adjacent lateral ligaments distal to the tibial ant joint line, no XR is needed to manage the patient.
Part of the rational behind this is that fractures not detected under this rule are minor and do better treated conservatively anyway. I like this principle! Nice to see a study evaluating the cost consequences of the implementation of a CDR. Few CDRs make it to this stage of impact analysis. They implemented the new rule at three different Canadian EDs and compared costs with three similar EDs doing usual practice.
Looked at costs up to 28 days after injury. In the 2000 or so kids in the study they found healthcare costs reduced by $37 per patient at intervention sites. The cost saving was mainly due to leave ankle XRs. As an aside there weren’t any more missed fractures in the intervention group (less in fact!) and use of the rule didn’t cause any extra follow-up.
In my experience most kids turning up to the ED reporting ankle pain get an XR at triage regardless of clinical signs. Those that don’t often end up getting one later from the doc as the parents really came for that above all else- I’m definitely guilty of this! If you were to implement this rule locally you would need to make sure your conservative treatment was similar to Canada, with similar follow-up. The most common treatment was elastic bandage and crutches, but moonboots, casts and splints were used. Follow-up seemed pretty similar to our practice. However for me rather than implementing formally I think this study can just make our decision better informed. Kids with pain but no swelling are the lowest risk of this low risk group. This is evidence their ED care can be safely streamlined without huge investment in the implementation of new rules. The benefit is that we better educate the public in what injuries need XRs and it frees up time and space for other EM care.
Further reading:
- Annals of EM Podcast (original source for this)
- Original Boutis paper
Paper Number 6

Click to go to PubMed
Observational paper to see if USS looking for the rapid atrial swirl sign to confirm central line placement. CXR was gold standard here. There were only 4 misplacements and USS identified 3 of these. With such small numbers of the outcome of interest it’s hard to know how good this would be.
Further Reading:
—
Subscribe: | RSS Feed